It sounds a bit trite, but it’s true nonetheless: the best type of exercise when you’ve got PD is any kind of exercise you’ll actually do. Fortunately, just as Parkinson’s disease presents in a wide variety of ways, there is a wide, wide range of exercise types that can help you manage your Parkinson’s symptoms. Surely you can find something you like?
A great place to start is with Make Your Move, a reader-friendly, thoroughly researched publication of the Michael J. Fox Foundation. (See ‘Selected Resources’ list at bottom for additional links.) With clear text and inspiring first-person stories, Make Your Move can get you started on a personalized exercise path to taking control of your symptoms.
+++++
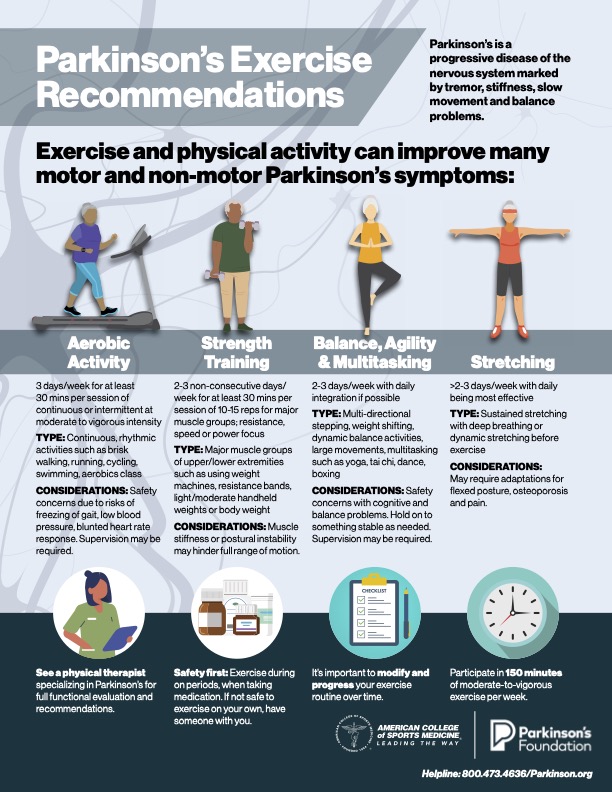
A picture is worth 1,000 words (even if the somewhat wordy graphic from the American College of Sports Medicine below already looks to have 999 or so…):
My motivation to exercise is pretty straightforward: On days that I exercise I feel more alert and engaged with the world. Sometimes I even feel like my old self (well, almost). And I sleep better, too, which gives me a big boost the following day.
Here’s my own (idealized) exercise regimen, adhered to as strictly as time, energy, and willingness on a given day allow:
Aerobic activity: Lots of walking and run-walking, aiming for 10,000 steps (+/- 4 miles) a few times a week. When weather and/or failing old-guy joints intervene, I supplement with an exercise bike.
Strength training: I usually lift weights twice a week at a health club. (I’m still fairly strong for an old coot, but that “fairly” is a pretty big qualifier…). I rotate upper and lower body exercises, and move quickly enough through my reps that my heart rate sometimes gets up into the high-intensity range. I keep lobbying my neurologist to let me count this as an aerobic activity, too, but she’s not budging. (“I know you love your weightlifting, Mark, but…no.“)
Balance, Agility & Multitasking: I cannot praise boxing, specifically the Rock Steady Boxing program, enough. It combines agility and balance with the joy of shouting at, and whupping the tar out of, a boxing bag. (Bonus feature: you don’t actually have to get hit.) Seriously, if you have PD and can find a Rock Steady program near you, sign up! I have similar praise for dance, specifically ballet, which I do once a week, and of which I have waxed poetic in past posts.
Stretching: Lordy, I’d love to stretch less often! I have problems with restless leg syndrome, which on bad nights can wake me up a half dozen times; stretching helps temporarily alleviate the weird, heebie-jeebie sensations that come with RLS. So, yes…I stretch.
Okay, up and at ’em! Hopefully this information will help get you started on a sustainable exercise program. And if (more like when) you fall off the exercise wagon, climb back on as soon as you’re able. Your Parkinson’s isn’t going anywhere!
There’s a young man who’s been working out at my health club for a few months now. When I first saw him he was sapling-skinny, with scarecrow hair, owlish eyes, and black, square-ish, never-in-style eyeglass frames. I had sympathy for him—I took care of a lot of teen boys wrestling with body image issues in my pediatric career. Dressed in baggy sweats, he could have been the inspiration for one of those 1950s Charles Atlas bodybuilding ads—the 97-pound weakling who gets sand kicked in his face by the muscle-bound beach bully (1):
And sure enough, just like Atlas’s scrawny “Mac”, the young man at the health club soon transformed his body. His determination was a thing to behold, as he followed an exhausting routine of curls, bench presses, squats, pull-downs, and more, adding a bit of weight to the bars each week. His broomstick arms sprouted biceps that steadily grew; pleased with his own progress, the young man took to striking furtive poses in the mirror that covers the back wall of the weight room.
He’s now well on his way to becoming a true Charles Atlas “new man.” Where he once crept into the weight room, he now strides in with confidence. His t-shirt has gotten tighter in the chest and biceps. He’s weed-whacked his hair into a fashionable ‘do’. He’s even got new, au courant glasses. Woe betide the bully who inspired this transformation—he’s in for a good girlfriend (or boyfriend)-witnessed chin-bopping sometime soon:
A righteous ‘bop’…
I’ve had to fight the urge to share my Parkinsonian learning with the young man. I’d like to tell him that all that iron he’s been pumping has made his brain stronger, too. Why, he’s got a zillion new neural connections all over his noggin – in the basal ganglia, the zona pellucida, the locus ceruleus, you name it! But he’s a twenty-something guy; who cares how good your brain looks at that age? I figure he’d just take me for a crazy old man. Which, I am.
+++
Here’s an old adage that I just made up: What’s good for the body is good for the brain. It’s true, if maybe not too catchy. When it comes to Parkinson’s, vigorous exercise of any kind, whether running, swimming, brisk walking, cycling, boxing, dancing, strength training à la Charles Atlas—basically, any form of exercise that gets your heart pumping—actually stimulates the growth of new neurons (brain cells) and strengthens connections between neurons in many parts of the brain. This makes for speedier and more efficient communication between areas of the brain, something of great importance to those of us with Parkinson’s.
But, really, there’s no anti-Parkinson’s magic going on here. Moving your body is good for all brains, not just the PD kind. The mechanisms behind the benefit are the same for the afflicted and the un-afflicted alike. It’s just that those of us with PD are starting in a neurological hole—we’ve been losing dopamine-secreting neurons for years, maybe even decades, before we’re diagnosed. Exercise can help you dig your way out a bit, or at least slow down the rate of decline.
How does exercise work its magic on the brain?
I learned back in high school biology that the adult brain was more or less a done deal, a mysterious, gelatinous blob that bossed around the body via an old-school scheme of stimulus and response. You were born with a finite number of neurons in your brain; our teacher told us, and once they’re gone, poof, they’re gone for good. I remember even then thinking that didn’t seem quite right—if head injuries or strokes destroyed brain tissue for good, I wondered, how did some people learn to walk or talk again afterwards?
When I reached medical school, I learned that, rather than a rigid, finished product, the brain was in fact plastic. (No, not in the single-use-shopping-bag sense; neuroplasticity is defined as the ability of the nervous system to reorganize itself, to change its structure, functions, or connections after injury or in response to external stimuli.) The brain has a remarkable—but not unlimited—capacity to heal itself.
The principle of neuroplasticity is critical to brain health in the neurotypical (aka, “normal”) individual and even more so in people afflicted with Parkinson’s disease. There’s currently no cure for PD—no way to undo the damage that’s been done by whatever the heck is causing the disease—and available medications provide only symptomatic relief. Exercise, though, can actually slow PD’s inexorable march. That’s why every newly diagnosed PD patient hears a nearly constant mantra from neurologists, therapists, and everyone else in PD world: You gotta get moving, bud!Movement is medicine!
And they mean “get moving” quite literally, because body movement sends a signal to both the neurotypical and PD-afflicted brain to crank out increased amounts of a molecule known as brain derived neurotrophic factor (BDNF). BDNF in turn stimulates the growth of neurons in areas of the brain that are active. It’s nature’s way of building up the neuronal pathways that a healthy body uses most, while not wasting energy on those that are neglected.
Of particular importance for people with PD, movement-stimulated BDNF production promotes the growth of neurons that manufacture dopamine, the neurotransmitter that controls and fine-tunes muscle activity and coordination. (Low levels of dopamine are responsible for the tremors, slowness, and rigidity characteristic of PD.) A virtuous cycle is thus created: body movement increases BDNF and dopamine production—especially in areas of the brain that control movement and balance—which in turn make it easier for you to move, which then stimulates the brain to produce more BDNF and dopamine…and so on. It’s a variation on the old saying, “use it or lose it”: Use it (move your body!) andgrow it (dopamine production).
What type of movement or exercise is best?
Good question! But this post has gotten pretty long, so how about I answer that one in my next post?
Stay tuned!
—–
Footnote:
1) Charles Atlas (1892-1972) was born Angelo Siciliano in Calabria, Italy. He emigrated to New York, in 1904, where as a teenager he became fascinated with the bodybuilders and strongmen at a Coney Island circus.
Atlas (he legally changed his name in 1922 after being told he resembled the statue of Atlas atop a Manhattan hotel), a late bloomer, described himself as the original “97-pound weakling” who got himself doubly humiliated one day when a muscle-bound guy kicked sand in his face at the beach as his girlfriend looked on and ridiculed him. Vowing revenge, Atlas whipped himself into muscle-man shape, a transformation that earned him a) the aforementioned revenge, in the form of a beach-bully beat-down; b) a job as a bodybuilder on Coney Island, c) a string of titles, including “America’s Most Handsome Man” and “America’s Most Perfectly Formed Man” and d) a lucrative side gig as a sculpture model. (Among many other artistic commissions, he posed for the statue of Alexander Hamilton that still stands outside the U.S. Treasury building in Washington, D.C.)
Charles Atlas is probably best remembered today for the wildly popular, full-page comic book advertisements for his eponymous body-building course. The story line in the ads hardly changed over the decades: a scrawny, dweeby-looking young man (typically named “Mac,” “Joe”, or “Jack”), dressed in ill-fitting, high-waisted swim trunks, sits with his shapely girlfriend on a beach towel, when, seemingly out of nowhere, a macho bully insults him (“Hey skinny! Yer ribs are showing!”), slaps him, and then kicks sand in his face, while Joe’s girlfriend snickers and further deflates his ego (“Oh, don’t let it bother you, little boy!”). Joe stomps angrily home, kicks a chair, vows revenge, then sends in a coupon for a free Charles Atlas booklet, and –lo!–two panels later he’s back on the beach with muscles popping out all over the place, bopping the bully in the jaw to the lusty approval of his fickle girlfriend (“Oh, Joe!” she coos as the bully skulks away. “You are a real he-man after all!”)
But a moral conundrum is left hanging in the air: Did Charles Atlas really make Joe a better man, or did he just create a new bully?
Some diseases are easy to diagnose. Take chickenpox—back in the day, before chickenpox vaccine became popular and case numbers plummeted, I’d see itchy, rashy, feverish kids several times a week during the winter and early spring. The stories were consistent: fevers for a day or two, then came the rash – dozens of small vesicles (thin-walled blebs filled with a watery fluid), each one on a red base.*
Quick, name that rash! (Hint: it’s not Parkinson’s)
I’d typically see the kids about 4 days into the rash, when the fevers and itchiness were driving everyone batty. I’d check for secondary bacterial infections and we’d discuss comfort measures that can make waiting out the illness less awful for both sick child and sleep-craving parent. Barring any unusual complications, things were better in a few days, and the scabby young victim now had lifelong immunity. Easy diagnosis, predictable stuff.
“The first essential criterion [in diagnosing PD] is parkinsonism, which is defined as bradykinesia and at least one of these two: a resting tremor or rigidity.” **
(Bradykinesia is defined as “reduction in speed and amplitude of voluntary movement.” This is much more than just slow walking. It includes such things as tiny handwriting that gets even smaller as the person writes; decreased facial expressiveness; weak voice; less frequent blinking; decreased arm swing when walking; and difficulty with dressing and with turning in bed.)
So, if you’ve got a slow-moving, retired pediatrician with either shaking limbs or unusual stiffness you’re looking at a guy with PD, right?
Not so fast…
What you’ve got so far is parkinsonism; you haven’t diagnosed Parkinson’s disease – at least not yet. PD is the most common neurologic condition that causes parkinsonism, but it’s far from the only one. So, once you clear the parkinsonism hurdle, you’ve got the rest of the Movement Disorder Society’s diagnostic criteria to consider: Supportive Criteria, Absolute Exclusion Criteria, and Red Flags. (Again, see Table 1. I never said this would be easy…)
Supportive criteria:
These are signs and symptoms that are often found in people with Parkinson’s but are not required to make the diagnosis. They include the effects of taking a “dopaminergic” medication (levodopa, for example)– is there a “clear and dramatic response?” Does the patient experience dyskinesia as a side effect? Other supportive criteria include the loss of the sense of smell and evidence of PD-related heart disease.
Absolute exclusion criteria:
The name says it all. Absolute exclusion criteria can exclude PD from your diagnostic possibilities…absolutely. The criteria include a number of complex neurologic features that would point to other diseases; taking medications that are known to cause parkinsonism (e.g., some seizure medications); not improving despite taking high doses of dopaminergic medications; having a normal PD-related brain scan; and (the neurologist’s wild card) an expert’s opinion that something else is going on.
Red flags:
These are signs and symptoms that may warn of something other than PD, but aren’t quite definitive in and of themselves. Among them is another batch of complex neurologic signs and symptoms that boil down to this: if your symptoms progress too quickly or too slowly (or not at all); if you fall down or faint a lot; if your symptoms are symmetrical (PD usually affects one side of the body more than the other); or if you’re not having sleep problems, constipation, psychiatric problem, and a host of other non-movement-related symptoms within 5 years of your diagnosis…maybe you don’t have PD after all.
Final score:
If your neurologist finds that you have parkinsonism, plus at least two supportive criteria, and no red flags or absolute exclusion criteria, you’ve got “clinically established PD.” If your supportive criteria exceed your red flags (of which there can be no more than two), you are considered to have “probable PD.” And if you have more than 2 red flags or any absolute exclusion criteria, you most likely have something other than PD. Back to the diagnostic drawing board with ye!
As you can see, it’s complicated. That’s why it can take weeks, months, sometimes even years for a slowly progressive disease like PD to declare itself, and why you really need a neurologist – even better, a neurologist who specializes in movement disorders like PD – to help you get an accurate diagnosis. (Retired pediatrician = not the guy you’re looking for.)
Coming up in the “Parkinson’s – the Basics” series: Now that you’ve got your diagnosis, you may ask yourself, “What is Parkinson’s disease, anyway? And why did I get it?” And the biggest question of all: “What’s next for me?” Answers (or at least some answers) to follow…
_____
* The classic description of the chickenpox lesion – “a dewdrop on a rose petal” – harkens to a more poetic medical era.A more accurate description: “An unattractive, sometimes yellowish bloblet plopped on a tiny patch of red skin. When it hasn’t been scratched beyond all recognition, that is…”(Copyright: me)
**Sometimes a picture really is worth a thousand words – click on link at bottom for a concise discussion of these three cardinal features of PD:
Bradykinesia(see in post above)
Resting tremor: “…slow, regular movements of the hands and sometimes the legs, neck, face, or jaw, when those parts are at rest; the tremor usually stops when that part is voluntarily moved.”
Rigidity: “…a stiffness of the arms or legs beyond what would result from normal aging or arthritis. Some people call it ‘tightness’ in their limbs.”
There are two main types of rigidity: “lead pipe rigidity,” which presents as a smooth resistance to movement of the limb, and “cogwheel rigidity,” which is a ratchet-like jerkiness superimposed on lead pipe rigidity.
If my blog had a title like “A Broken Leg,” explaining my medical woes would be so much easier. What’s my condition, you ask? Why, it’s right there in the title: I broke my leg. How did I get it? I slipped on a banana peel, maybe, or proved that there is such a thing as “too old to learn to rollerblade.” How do you treat it? You slap a hunk of plaster on it and then wait. What are my chances of complete recovery? Pretty good, if I stop buying Safeway bananas and sell my rollerblades on eBay pronto.
But, no…I had to go and get a disease that can take years to diagnose, is highly variable in its symptoms, and can involve pretty much any body system you’d care to name. The etiology – the medical term for the reason I got it in the first place – can be genetic, or related to toxic exposures, or recurrent head injuries, or some combination of things. Or just bad luck. The treatment is complex, involving an often mystifying array of medications, brain implants, therapies (physical, occupational, speech, psycho), and exercise – everything from ballet, to tai chi, to boxing. The chances of complete recovery? Slim to none. Frankly, I’d rather have a broken leg. Maybe six.
But, hey, this is a Parkinson’s journal, so in upcoming posts in this series I’ll try to explain the medical intricacies…